
Jobs vs lives: the tough decision governments have to make
When you compare our COVID-19 experience to that of other countries, it’s clear that our governments – at all levels – have done a stellar job in keeping almost all of us safe. They’ve done this by shutting down much of our economy. But now they’re faced with the inevitable dilemma: how soon to open it again?
We have for a week or so believed that the narrative would swiftly shift towards unlocking the lockdown and that certainly appears to be the case. A chart (figure 1.) published in The Australian Financial Review provides not only food for thought, but also a roadmap for the public to digest.
In another blog post we have written:
“The most confounding decision to soon confront governments will be the one that requires them to decide how the greater good is best served. Is it best served by saving all lives or is it best served by allowing some to die in order that the majority may get back to generating economic units of output? Minimising virus deaths and restarting the economy is also the most vexing question for investors.
I believe however that question is already being answered in the public domain. A staged return to work is not only inevitable but I currently believe likely to begin sooner than previously indicated.”
Figure 1. The Australian Financial Review
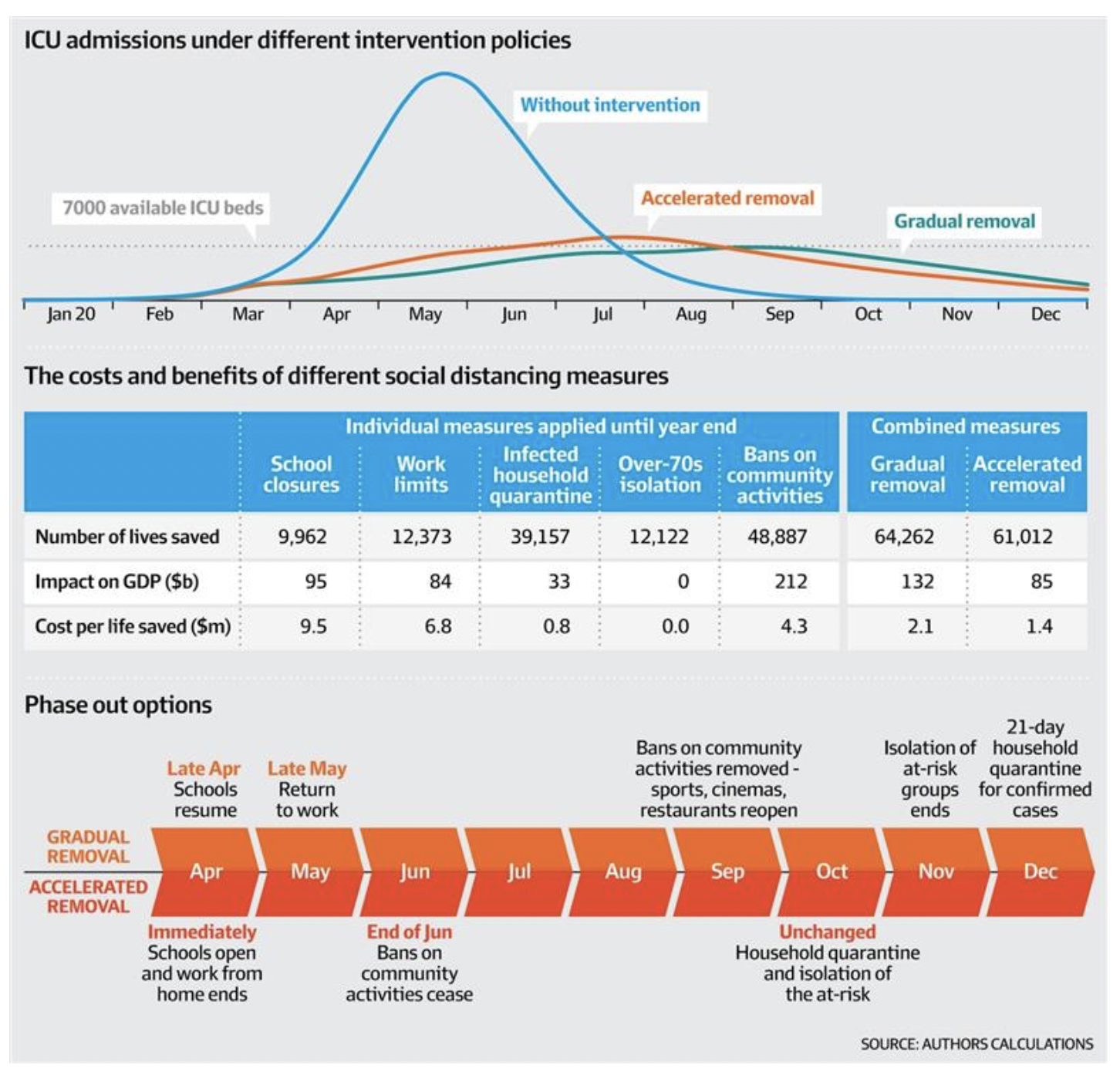
We think the government are trying to get ICU beds up over 10,000. We believe they have an inventory of 5000 ventilators today with another 5000 on order, presumably arriving soon. This provides for a scenario that allows the ICU and ventilator capacity that the Australian Medical Journal reported on, to come into play and for herd immunity to be developed. That requires 15 million of us to contract the virus and around 10,000 of us at a time needing ICU support. It hardly sounds like a dream plan, but it allows economic activity to resume to a level, while unknown, a whole lot closer to normal than we are operating at today.
Will they do it? That depends on the public’s acceptance. The fit, young and strong will push for it. The elderly and frail will deem it dangerous and foolhardy. The government has accumulated some political capital through the sound management of the outbreak today and so can afford to spend a bit on populism.
Here’s an issue though. If one assumes an ICU bed is used by one patient for one week (the Doherty model assumes a 10 day stay in ICU) then it can support 520,000 patients a year at maximum capacity. At an ICU/hospitalisation rate (hospitalisation rate is not ICU rate, see NSW paragraph below) of say five per cent, that would be 10.4 million people contracting the virus per year or 28,500 a day. Even at that rate it would take 18 months to get to the 60 per cent minimum for herd immunity. And we are a long way from 28,500 a day contracting it.
Another point is that herd immunity depends on people actually becoming immune after contracting COVID-19. An article by Bloomberg this week, interviewing quite a few experts, suggests it is not clear immunity occurs after recovery in the case of COVID-19. Different coronaviruses offer very different length of immunity after infection.
NB: Currently there are 29 people in NSW ICUs and 18 on ventilators. Assuming these are all people diagnosed in the last two weeks (of which there were 704 in NSW) that is 4.1 per cent ICU admission rate and 2.6 per cent ventilator demand rate respectively. Obviously, this isn’t a large sample so there would be a big error around this to the actual mean. And if the average stay is 10 days rather than 1 week, the annual capacity is 50 per cent short, and the amount of time to get to herd immunity will be 50 per cent longer.
A lot for our government to seriously consider.
Roger Montgomery is the Founder and Chairman of Montgomery Investment Management. Roger has over three decades of experience in funds management and related activities, including equities analysis, equity and derivatives strategy, trading and stockbroking. Prior to establishing Montgomery, Roger held positions at Ord Minnett Jardine Fleming, BT (Australia) Limited and Merrill Lynch.
He is also author of best-selling investment guide-book for the stock market, Value.able – how to value the best stocks and buy them for less than they are worth.
Roger appears regularly on television and radio, and in the press, including ABC radio and TV, The Australian and Ausbiz. View upcoming media appearances.
This post was contributed by a representative of Montgomery Investment Management Pty Limited (AFSL No. 354564). The principal purpose of this post is to provide factual information and not provide financial product advice. Additionally, the information provided is not intended to provide any recommendation or opinion about any financial product. Any commentary and statements of opinion however may contain general advice only that is prepared without taking into account your personal objectives, financial circumstances or needs. Because of this, before acting on any of the information provided, you should always consider its appropriateness in light of your personal objectives, financial circumstances and needs and should consider seeking independent advice from a financial advisor if necessary before making any decisions. This post specifically excludes personal advice.
The other factor to consider is what percentage of the population are asymptomatic? There have been 2 studies out of the USA suggesting that many, many more people have been infected but don’t show symptoms. If proven, this would mean Coronavirus is far less deadly and it will be far quicker and easier to achieve herd immunity.
Yes we are aware Ricky, Santa Clara and LA County.
1. ICU beds and ventilators are are only scaleable as the operators/nurses/ doctors who can safely operate them, deeper training is required in these areas. Federal and state authorities are now becoming aware that there are not nearly enough trained staff to opertate double the ICU beds and associated hardware required and will become available.
2. More interesting is there is a larger than expected number of trained medical staff who have chosen to make themselves unavailable for work due to the higher threat levels at hospitals and gp clinics.
The models currently assume a 1:1 linear response…flawed assumption, try modelling the available and trained staff numbers who are actually available.
Thanks George.
The argument, going about, for going for herd immunity does not make sense. We still have no idea about the pathology of this virus – maybe with each repeated infection it gets worse, maybe it is able to remain latent and emerge at a later date. The extent of pathology may relate to dosage – one might get infected one time an recover easily and then another time be badly hit. Even the issue with respirators is complicated as the virus seems to be attacking blood vessels rather than being a pneumonia blocking the oxygenation . In my view the lock down is giving us more time to understand what is going on and the big mistake of people trying to open the economy up is to assume that this is like a bad flu and we need to just accept the risk- this virus may well be more like HIV, dengue or herpes than the flu and we need to be very careful that we actually know what we are dealing with.
Thank you John. These are helpful insights.